More than 90,500 new consumers selected a plan through Nov. 30.
While plan selections are ahead of the pace set in 2016, when Covered California also delayed its marketing until after Election Day, they are slightly behind the pace set during 2017.
Roughly 1.2 million Covered California enrollees have been renewed for 2019, similar to last year’s totals.
An estimated 1.1 million uninsured Californians are eligible to enroll in Covered California or Medi-Cal. New research shows that 82 percent of uninsured consumers surveyed, who are eligible for financial assistance, do not know that they qualify.
Consumers must sign up by Dec. 15 in order to have their health insurance start on Jan. 1, 2019. Open enrollment in California continues through Jan. 15.
DENVER — More than 46,000 Coloradans selected health coverage through Connect for Health Colorado® during November, a number 6 percent ahead of the pace one year ago, according to new data released today.
“We started with a strong month but there are now only 12 days left to get coverage in place for Jan. 1,” said Connect for Health Colorado® CEO Kevin Patterson. “It is time for Coloradans who buy their own health insurance to act to protect their health and their family finances.”
During November, Connect for Health Colorado customers made 46,332 medical plan selections. The total was 43,881 medical plan selections for the comparable period in 2017.Fifteen percent of the plan selections are by customers who are new to Connect for Health Colorado and 85 percent are renewing customers.
Two weeks ago I reported that Access Health CT, Connecticut's ACA exchange, had enrolled 12,777 people in 2019 ACA exchange policies, running neck and neck with last year. This included active renewals and new enrollees only.
HARTFORD — Enrollment in Access Health CT is higher this year than it was last year at this time, but time is running out.
Officials said they’ve enrolled 9.685 customers who are new to the exchange this year, and they’ve auto-enrolled more than 91,000 customers who purchased plans with them in 2018. That brings total enrollment up to 101,054 individuals as of Nov. 30.
Last year, about 90,428 individuals had enrolled by this time.
A couple of weeks ago I reported that the Washington Health Benefit Exchange reported enrolling a seemingingly astonishing 190,000 people into 2019 policies in just the first 10 days of the 2019 Open Enrollment Period. This is highly misleading, of course, because only a small fraction of these are new enrollees, and a somewhat larger portion are current enrollees actively renewing their policies.
The vast bulk of that 190K are current enrollees who are auto-renewed into 2019 policies by the exchange itself...with the option to then actively go into the system and opt to cancel their renewals if they wish. There's nothing wrong with this, and in fact more and more of the state exchanges seem to be doing it this way as they improve and streamline their software (I've confirmed that Maryland, Massachusetts, Minnesota, Rhode Island and Washington State are "front-loading" autorenewals this year, although Maryland hasn't actually reported their data yet).
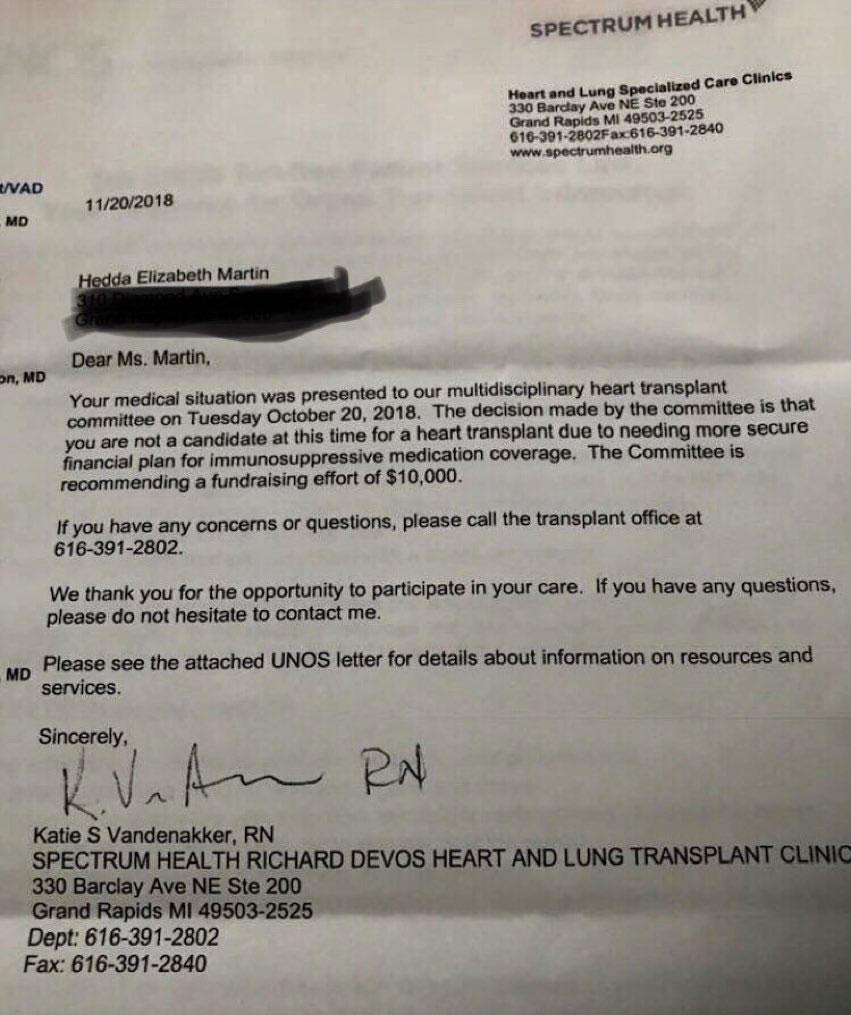
Earlier this week, a picture of a letter sent to a patient needing a heart transplant recommending that they find a way to raise $10,000 to cover some costs went viral on Twitter and Facebook, with various celebrities, politicians etc. reposting it.
I'm sure you've seen it already, but just for the record, here's one of the most viral variants, from freshman Congresswoman-elect Alexandra Ocasio-Cortz. It's important to clarify that the letter was not sent by the insurance carrier, and the $10K in question would not be going to pay an insurance company...or, in fact, even "Spectrum Health" aka the "Heart & Lung Specialized Care Clinics" noted in the letterhead.
Insurance groups are recommending GoFundMe as official policy - where customers can die if they can’t raise the goal in time - but sure, single payer healthcare is unreasonable.
PROVIDENCE — HealthSource RI, the state’s health insurance exchange, reports 31,000 people have signed up for health care coverage about a month into the open enrollment period for the 2019 plan year ending Dec. 23, 3,600 enrollments ahead of where they were at this point last year.
Last year at about this time during open enrollment, HealthSource RI had counted about 27,400 people enrolled for health insurance through the exchange, according to HealthSource RI Director Zachary W. Sherman.
Sherman said the agency has seen many people renewing existing coverage either manually or automatically.
“We’re pleased with where we are with sign-ups,” Sherman said.
A month ago I posted a Red Alert about the latest regulatory attack on the ACA...this time coming directly from CMS Administrator Seema Verma. At the time, Verma had just announced a draft version of the new rules for Section 1332 Waivers...starting with changing the name from "State Innovation Waivers" to "State Relief and Empowerment Waivers", which sounds in no way like Orwellian doublespeak propaganda.
Here's the basic backstory on 1332 waivers:
One of the great strengths and dangers of the ACA is that it includes tools for individual states to modify the law to some degree by improving how it works at the local level. The main way this can be done is something called a "Section 1332 State Innovation Waiver":
A couple of weeks ago I noted that the Illinois state Senate unanimously overrode outgoing Governor Rauner's veto of their bill restricting the sale of non-ACA compliant short-term, limited duration healthcare plans.
Today, I'm happy to report that the state House has followed up and overrode the veto as well:
Breaking: Just got word that the Illinois legislature has overridden the veto on SB1737 which limits short term plans to 6 months and bans rescissions of short term plans. @GtownCHIR h/t @stephanibecker
This report provides average effectuated enrollment and premium data for the Federal and State-Based Exchanges for the first six months of the 2018 plan year. The Centers for Medicare & Medicaid Services (CMS) publishes effectuated enrollment data semiannually to provide a more accurate picture of enrollment trends for the Exchanges than indicated by the number of individuals who simply selected a plan during Open Enrollment. For coverage to be considered effectuated, individuals generally must pay their premium for the given month.